




Patent Ductus Arteriosus (PDA) - Causes, Symptoms, Diagnosis
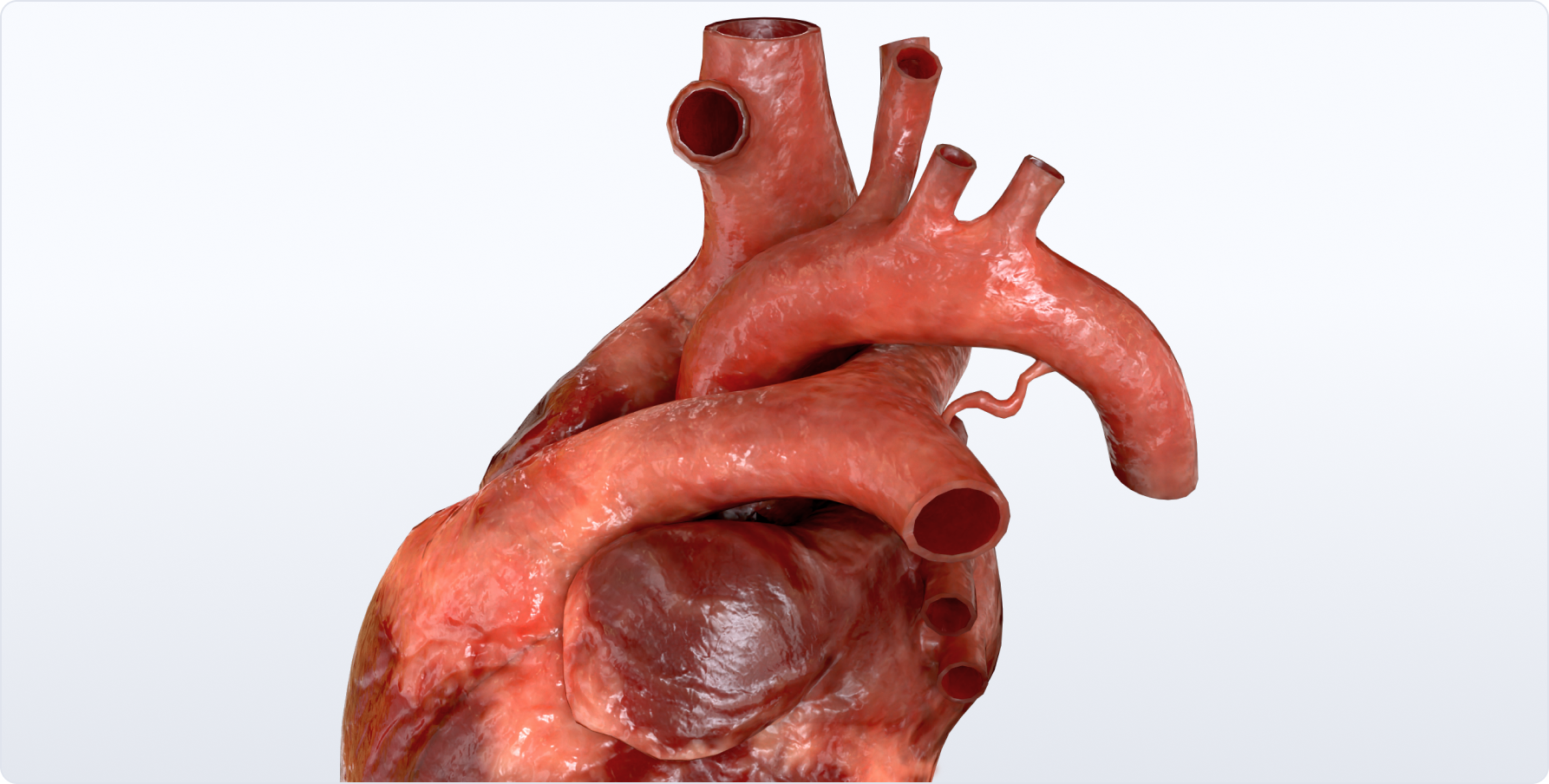
Table of content
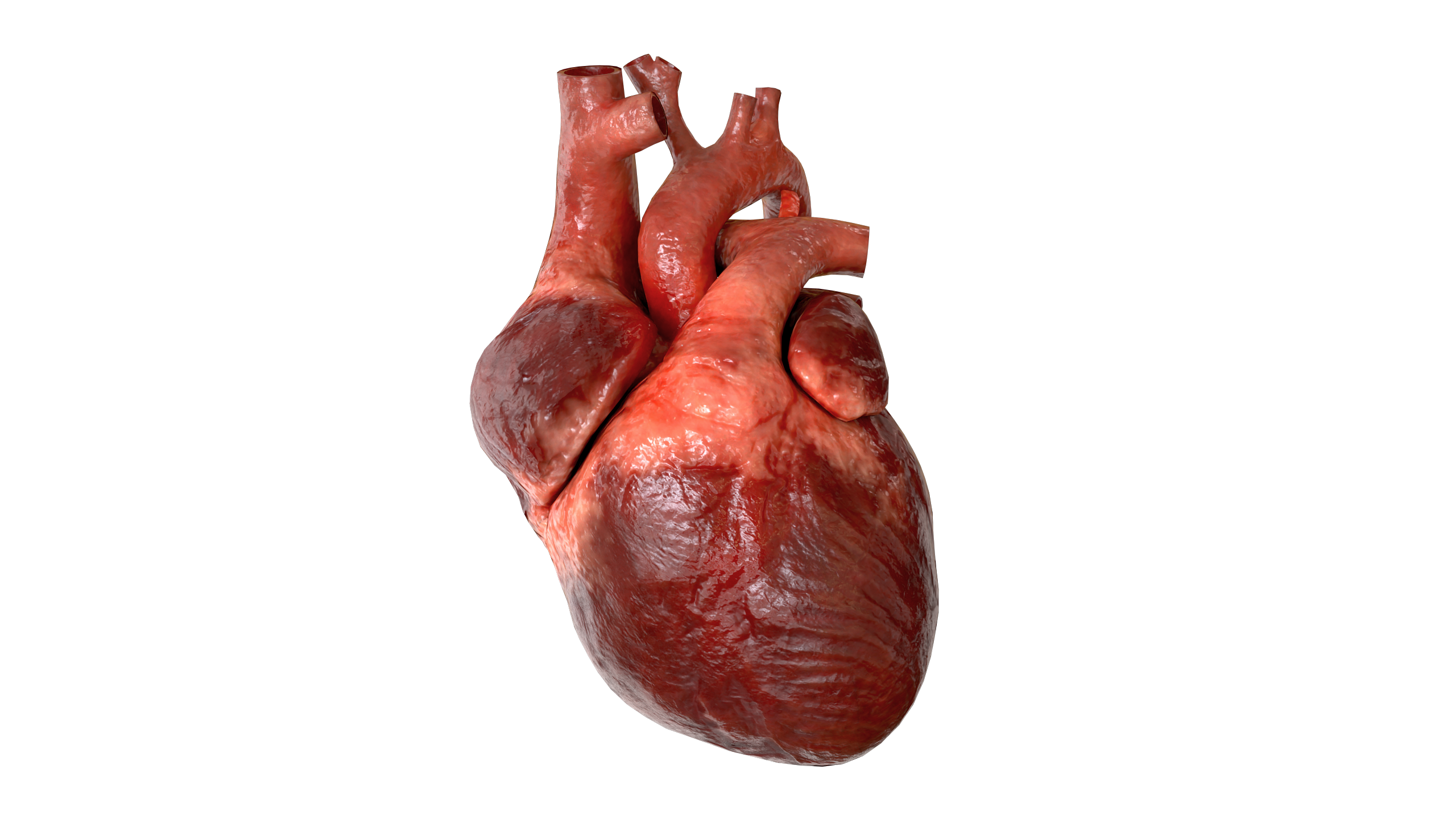
Patent ductus arteriosus is a congenital heart defect in which the ductus arteriosus remains functional after birth.
Embryology
The arterial duct arises and forms along with the division of the common arterial trunk. During fetal life, the ductus arteriosus is a normal structure that allows most of the blood leaving the right ventricle to bypass the pulmonary circulation and pass into the descending aorta. Normally, the ductus arteriosus closes within a few days after birth due to lack of functional need.
Anatomy
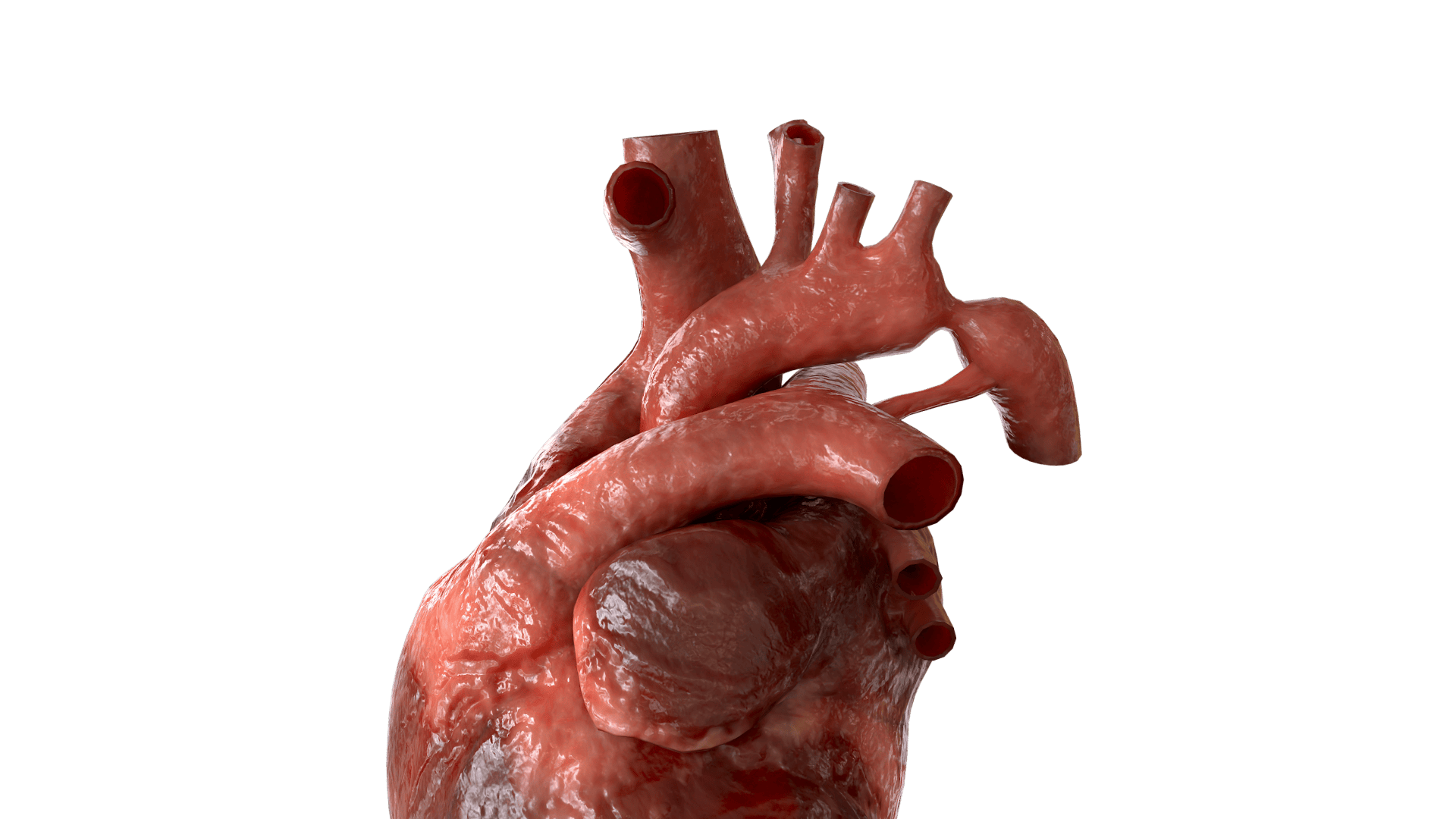
Most frequently, the arterial duct departs from the aorta slightly below the left subclavian artery, and then approaches left pulmonary artery. Typically, the ductus has a conical shape with a large aortic end tapering into the small pulmonary connection.
Classification
Conical;
Window-shaped;
Tubular.
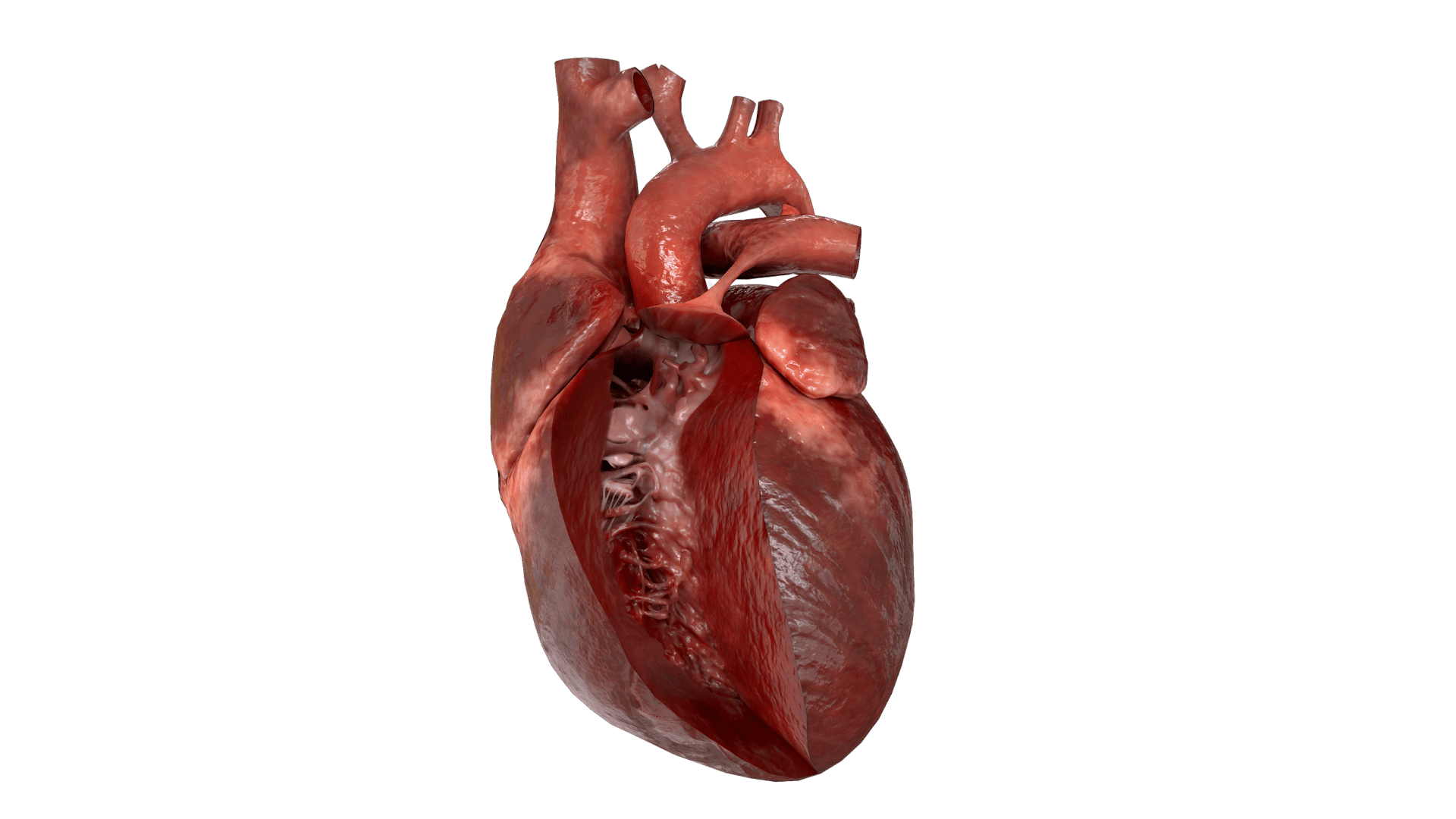
Hemodynamics
Systemic circulation is mainly carried out through the ductus arteriosus: blood is shunted from the nonfunctional pulmonary system into the descending aorta. The first breath of the newborn initiates the flow of blood into the pulmonary system. Over time, the resistance of the pulmonary vessels decreases, which leads to changes in bloodflow through the ductus arteriosus.
A large volume of blood goes from the aorta to the pulmonary artery under great pressure. The same volume of blood returns to the left heart, which results in left atrial and left ventricular enlargement. The magnitude of the excess pulmonary blood flow and relationship of the pulmonary vascular resistance (PVR) to the systemic vascular resistance (SVR) (Qp : Qs) depends on the size and shape of the duct.
Ultimately, a constant pulmonary overcirculation leads to the vessel wall remodeling and development of the pulmonary vascular obstructive disease (PVOD). After a significant increase of the pulmonary artery pressure, the direction of the shunt can change to right-to-left.
Workup
Doppler Echocardiography, CT. Visualization and differential diagnostics.
ECG. Has no diagnostic specificity.
Radiography. Not specific. Radiographic signs of pulmonary overcirculation are noted only after the development of pulmonary hypertension.
Cardiac catheterization. It is indicated in cases of a critical pulmonary hypertension to clarify its nature and possibilities of surgical treatment.
Clinical manifestations
Clinical manifestations depend on the size of the duct and the stage of hemodynamic disorders. The typical child with a patent ductus arteriosus is asymptomatic. Large patent ductus arteriosus can manifest within first days of life. Typical clinical signs of heart failure in such children will be: shortness of breath, tachycardia, feeding disorders, hepatosplenomegaly, and physical retardation. It is also may be associated with recurrent respiratory infections, atelectasis and pulmonary hypertension. When the direction of blood discharge changes, arterial blood from the aortic arch flushes venous blood from the ductus arteriosus into the descending aorta, causing primarily lower extremities cyanosis.
Typical signs include:
Continuous systolic-diastolic murmur in the ІІ – ІІІ intercostal space to the left of the sternum;
Decrease in diastolic blood pressure.
After the onset of pulmonary hypertension, the nature of the noise changes: the diastolic component of the noise decreases and then completely disappears.
Treatment
In premature infants, conservative management of patent ductus arteriosus is used. It involves the administration of indomethacin to obliterate the duct. In most cases, surgical treatment is indicated. Surgical treatment in newborns is indicated early in order to avoid irreversible heart and other systems complications (premature newborns are highly likely to develop NEC and renal failure). In case of the development of high pulmonary hypertension with pulmonary vascular remodeling, surgical treatment is contraindicated.
The following surgical techniques are used:
Catheter closure;
Surgical ligation and / or clipping which entails a thoracotomy.
External sources
Catalog VOKA.
https://catalog.voka.io/
Thapar, A., Jenkins, I. H., Mehta, A., & Davies, A. H. (2013). Diagnosis and management of carotid atherosclerosis.
BMJ, 346, f1485. Doi: 10.1136/bmj.f1485
Goethem, J. V., Hatsukami, T., Rothwell, P., Brown, M. M., & Moody, A. R. (2021). Roadmap consensus on carotid artery plaque imaging and impact on therapy strategies and guidelines: An international, multispecialty, expert review and position statement.
American Journal of Neuroradiology, 42(9): 1566–1575. Doi: 10.3174/ajnr.A6798
Naylor, A. R., Ricco, J.-B., de Borst, G. J., Debus, S., de Haro, J., Halliday, A., ... & ESVS Guideline Review Group. (2018). Editor's Choice—Management of atherosclerotic carotid and vertebral artery disease: 2017 clinical practice guidelines of the European Society for Vascular Surgery (ESVS).
European Journal of Vascular and Endovascular Surgery, 55(1), 3–81. Doi: 10.1016/j.ejvs.2017.06.021
Moore, K. J., Sheedy, F. J., & Fisher, E. A. (2013). Macrophages in atherosclerosis: A dynamic balance.
Nature Reviews Immunology, 13(10), 709–721. Doi: 10.1038/nri3520
Thank you for your comment!
Your comment has been submitted for moderation and will be published soon. We'll email you once it’s live.